


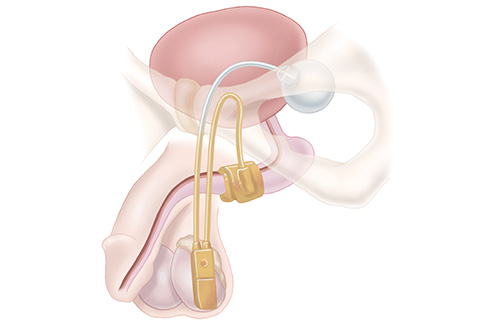
Artificial urinary sphincter (AUS) is the most common surgical procedure performed in men who leak urine after prostate cancer treatment. An inflatable cuff is placed around the urethra through a small incision under the scrotum.
It causes physical compression to limit urine leakage. Patients briefly squeeze a small control pump underneath the skin in the scrotum to deflate the cuff and urinate before the cuff automatically re-inflates. The fluid cycles between the cuff and a small reservoir placed through a small incision in the groin. AUS is appropriate for patients with moderate-to-severe stress incontinence in patients who have the manual dexterity to operate the control pump. The cuff can be deactivated by a Urologist if subsequent temporary catheter placement is needed but every attempt should be made to avoid future catheterization as this instrumentation could damage the cuff.
When to Ask a Urologist about Artificial Urinary Sphincter
You should speak with a Urologist about Artificial Urinary Sphincter if you have persistent urine leakage following prostatectomy and would be interested in learning about procedures that may be able to stop or decrease your leakage.
Cost
Typically covered by most insurances (although coinsurance and deductibles may apply). Coverage will be verified prior to proceeding. If you do not have insurance, our office will be able to give you an out-of-pocket cost estimate.
Effectiveness
About 75% of patients report using zero or one pad per day following AUS placement. The rate of persistent severe incontinence is low (9%).
Possible Side Effects
The various risks associated with the procedure include the possibility of persistent urine leakage, pain, bleeding, palpable reservoir, device malfunction, and damage to surrounding structures. The rate of revision surgery is about 28% at 5 years. The primary risks are infection (1-3%) or urethral erosion (5%) which would require removal of the device. You must avoid any catheter placement in the future unless directed by a urologist because attempts at catheterization while the AUS is in place may cause irreversible damage requiring device removal.
Alternative Approaches
Alternatives to AUS placement include observation without treatment, pelvic floor muscle physical therapy, penile clamp device, chronic indwelling catheterization, chronic condom catheterization, and male urethral sling placement.
What to do to Prepare for Surgery
You will receive detailed instructions from the surgical schedulers regarding any necessary testing or appointments prior to surgery. In general, you should temporarily stop blood-thinning medications prior to surgery (when to stop depends on the type of blood thinner). Prescription blood-thinning medications should be stopped following clearance from the doctors that prescribed them though other medications that thin the blood including fish oil and pain relievers such as ibuprofen should be stopped as well.
On the day before surgery, you will receive a phone call alerting you to the time that you should arrive, and you should wash the surgical area with an antibacterial soap.
You should not eat or drink anything after midnight on the day of surgery, but you may take approved home medications in the morning before surgery with a small sip of water.
What to Expect after Surgery
The procedure typically requires an overnight hospital stay with a catheter that is removed the following day. There is a small incision in the groin area as well as an additional incision underneath the scrotum. There can be significant tenderness, bruising and swelling that dissipates over 2-3 weeks. The device is left deactivated initially after surgery. Therefore, it is expected that urine leakage will continue in the postoperative period until device activation around 6 weeks following surgery.