


Benign prostatic hyperplasia (BPH) refers to an increase in the size of the center portion of the prostate.
The enlarging prostate gland can result in bothersome urinary problems called lower urinary tract symptoms (LUTS). The prevalence and degree of LUTS typically increases as men age and the prostate keeps growing with approximately 50% of men reporting moderate to severe bother by age 70. Symptoms from obstruction due to BPH typically include straining to urinate, slow stream, sensation of incomplete emptying, and waking up at night to urinate.
Know Your Score
Causes and Risk Factors
The process of prostate enlargement increases as men age and more greatly affects men with a family history of enlarged prostate. The underlying cause is not well understood.
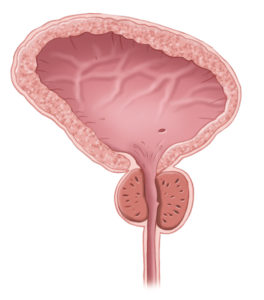
Normal Prostate
When to Speak with a Urologist about BPH
Whenever you are bothered by it! Just because it is common, does NOT mean you have to accept or live with it. LUTS primarily impact quality of life. The good news is it rarely represent a life-threatening condition such as cancer. However, it does often worsen as men age. In some cases, it can lead to permanent bladder damage and the need for catheters. So, talk to your Urologist as soon as your symptoms start to bother you!
What to Expect when Seeking Treatment
In addition to a history and physical examination, initial assessment includes urine testing to rule out infection and completion of the International Prostate Symptom Score (IPSS) questionnaire to quantify the symptoms. Additional evaluation such as measuring post-void residual to check for bladder emptying, uroflow and UroCuff are sometimes necessary to help create your treatment plan. A voiding diary for two or three days may be helpful to determine if you are producing more urine at night than is normal. In more complex cases, such as those considering procedural intervention and men who fail to improve with initial treatment, further testing with urodynamics, cystoscopy and ultrasound for prostate sizing can help you choose your best treatment options.
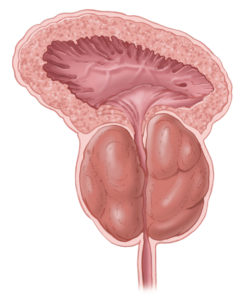
Enlarged Prostate
Treatment Options
This condition is too varied and complex for a one-size-fits-all approach. We are proud to offer a full variety of treatment options customized to your goals and preferences.
Lifestyle and behavioral modifications can improve LUTS. These conservative measures include:
- Compliance with CPAP use during sleep
- Limiting fluid intake particularly in the evening
- Avoiding bladder irritants such as caffeine and alcohol
- Modifying drug therapy such as morning diuretic administration and avoiding decongestants
- Avoiding constipation
- Sitting with legs elevated in the afternoon to reabsorb lower extremity fluid before bedtime.
Medical Options
Herbal supplements have not been shown to be effective in the treatment of LUTS and are generally not recommended. Initial medical management involves an alpha blocker drug (such as Flomax, Uroxatral and Rapaflo) that selectively relaxes the prostate muscle cells around the urethra. These medications improve IPSS scores by 5 points on average. Side effects include possible dizziness (about 5% risk), slight decreases in blood pressure, retrograde/lack of ejaculation (about 10% risk).
For men with large prostates (over 40 grams), adding a 5-alpha reductase inhibitor (such as Proscar and Avodart) can further improve LUTS and lowers the IPSS score by 3 points on average. These medications also reduce progression to surgery and worsening bladder function by about 50%. Side effects may include decreased libido (about 3% risk) and rarely breast tenderness / enlargement.
An additional medication option is daily Cialis which has been shown to improve IPSS score by about 4 points and has additional benefit of helping with erections. The mechanism for improving LUTS is unclear.
While most men with LUTS have blockage due to their prostate, overactive bladder can also contribute. Anticholinergic medications (such Ditropan and Vesicare) and beta-agonists (Mybetriq) can help to calm the bladder. Risks include the inability to urinate, dry mouth, constipation and high blood pressure.
Surgical Options
For men who prefer to avoid daily medications and their potential side effects, or for men with persistent bother and worsening bladder function despite medicines, surgical intervention can be appropriate. Other reasons your Urologist may recommend a procedure include renal insufficiency, recurrent urinary tract infections, recurrent gross hematuria or bladder stones.
Prior to surgical intervention, you and your doctor may determine additional tests such as uroflow, measuring post-void residual, urocuff, urodynamics, cystoscopy and ultrasound for prostate sizing are right for you to help determine how likely you are to improve after a procedure.
Transurethral resection of the prostate (TURP), which physically scrapes away the inner portion of the prostate, is one of the oldest and most well-studied procedural interventions for BPH. The average patient has an 18 point IPSS improvement and 15 cc/sec increase in maximum flow rate. This procedure requires a catheter for 1-5 days and an overnight stay in the hospital.
Laser prostatectomy (also called PVP, KTP or Greenlight prostatectomy) relies on a laser to vaporize the inner portion of the prostate and it has been shown to be non-inferior to TURP during the GOLIATH trial, a head to head comparison between the treatment modalities. This procedure has the benefit of lower risk of bleeding than TURP and can be used for patients on blood thinners. It typically does not require an overnight stay in the hospital. The average patient has a 70% reduction in their symptoms based on IPSS. Depending on the way your prostate has overgrown, laser prostatectomy may not be right for you.
Urolift represents a newer and less invasive approach. It uses tensioned implants to hold the lobes of the prostate apart, similar to pulling back window curtains. It improves IPSS scores by 50%. Although common after TURP and laser prostatectomy, the rate of new ejaculatory dysfunction after Urolift is approximately 0%. After Urolift only half of men need a catheter. When needed, it is typically only for 1 day. Since this treatment option is newer, there is less information available regarding long-term (greater than 5 year) effectiveness and need for repeat procedures.
Rarely, prostates are too large to be managed via these techniques and more invasive or advanced options such as robot-assisted/open simple prostatectomy or holmium laser enucleation of the prostate (HoLEP) are needed.
It is important to remember that bothersome urinary symptoms may be temporarily worsened for a few weeks to months following these procedures as inflammation subsides and the bladder adjusts.